Some of you will already know that I’m losing my motability car on the 23rd of April. I’m incredibly angry as this effectively leaves me housebound. So I’m having to spend money I can’t spare on buying an ‘old banger’ so I can get out.
So why is this happening?
- Because this govt don’t want people on disability benefits
- Because in conjunction with the MSM they have wrongly demonised disabled claimants as scroungers
- Because they’ve moved the eligibility goalposts to make it even harder to evidence disability
- Because their contracted “health assessors” (who aren’t experts in many conditions including mental health issues) are targeted on reducing benefit levels
- Because their contracted assessors blatantly lie, misinterpret & make erroneous assumptions in their reports which are then treated as gospel over claimant evidence, scans, & consultant correspondence
- Because they f*cking can & the MSM is complicit in covering up their lies

I know I’m not alone in this, I know other people who’ve been through this right to the appeal tribunal stage & won back their rightful benefits because at a tribunal you’re dealing with humans, not dwp targets. But I also know so many are just too ill, too tired, too anxious, too stressed, too alone, too defeated & too confused, and have given up without appealing even though they know they’d likely win. The fight is too hard & this govt are relying on that to cull numbers.
Almost a third of DLA to PIP claimants lose benefits, cutting their independence & their income. Disability charity Scope said these figures are “deeply concerning” and called for an “urgent overhaul” of the assessment process
“It’s deeply concerning that so many disabled people are facing a sudden drop in vital financial support,” said James Taylor from Scope.
“Life costs more if you are disabled. These extra costs haven’t disappeared just because there is a different assessment process.
“Without an urgent overhaul of the PIP assessment process, the system will continue to work against disabled people, instead of for them.”
I won’t go into my medical details here because much of it is very personal, but I cannot emphasise the following things enough;
The stress & anxiety have been absolutely horrendous. Imagine some unknown & unsympathetic stranger has complete control over your finances & your car, then imagine they won’t tell you for month after month what they’re doing next. I had my initial dwp letter in June last year. My assessment wasn’t until 1st December. I didn’t get a decision until February (and I had to chase them).
So I completed with Citizens Advice the initial Mandatory Appeal (which is known to be a pointless exercise but still took us two hours), unsurprisingly I’ve had a letter today denying the HR disability again & repeating what was said in the last letter almost verbatim. So next stage is to go to court for a legal Appeal Tribunal, which I understand from others can take up to a year.

My depression has absolutely been impacted by this process too, I’ve had more down days, the black dog nips a little closer when even thinking about not having reliable transport, & also of being accused of being a liar which is essentially what the dwp have done to me & thousands of other disabled people. I’ve been agitated & restless & I know exactly what the cause is.
My rage has settled down to a simmer now, but I was so bloody angry when I finally got my report copy. (Confession – I may have written certain rude words in pencil all over the margins). It’s outrageously poor.
Bear in mind here for a minute that in a previous life I ran huge contracts across the South West for (plot twist) the dwp, supporting the unemployed into work. The irony isn’t lost on me! But had any single member of staff in one of my centres turned in a report of this poor a calibre about a client some very serious conversations would have been had.
I’ve not picked it up for a few weeks because it’s still a bit raw, but off the top of of my head…. It’s a badly written cut & paste job, some of which obviously came from doing someone else’s assessment. It’s practically illiterate. The same phrases are repeated over & over like magic, as if when you say something stupid/untrue often enough it becomes reasonable or true. It contains as I said earlier outright lies, glaring inaccuracies and erroneous assumptions. There is no logic or consistency.
It took me a few days to work out that at least part of my anger was precisely because of the poor composition and lack of attention to the construct and meaning, as well as the errors. I know I’m a detail orientated person and these things matter to me, but surely in doing work that will actually impact people’s lives, wellbeing & financial circumstances everyone should pay attention to detail?
Almost a third of DLA to PIP claimants have lost benefits, cutting their independence & their income. Disability charity Scope said the figures are “deeply concerning” and called for an “urgent overhaul” of the assessment process.
“It’s deeply concerning that so many disabled people are facing a sudden drop in vital financial support,” said James Taylor from Scope.
“Life costs more if you are disabled. These extra costs haven’t disappeared just because there is a different assessment process.
“Without an urgent overhaul of the PIP assessment process, the system will continue to work against disabled people, instead of for them.”
Call me naive, but I guess I expected better from a government employed organisation when producing an official report on someone’s mental & physical health & ability. So yes, on top of everything else I was actually incredibly disappointed.
In my previous life with a fully functioning brain I would have torn this report to shreds in a couple of hours, referring to the DWP’s own guidance point by point to emphasise each and every error. Unfortunately with frequent brain fog, cognitive difficulties & fatigue unpicking this to refute it for a tribunal will take me weeks. But if needs be I will do so, with the support of friends, and the fabulous Citizens Advice, because even feeling as ill as I do daily I’m too bloody angry & stubborn to let this go.
I hope the above has made sense, I’ve probably rambled but this is the first time I’ve felt calm enough to write this out without ranting &/or swearing (a lot)!
Thanks to everyone who’s supported me, especially the lovely Essia who attended with me in December to literally & metaphorically hold my hand.
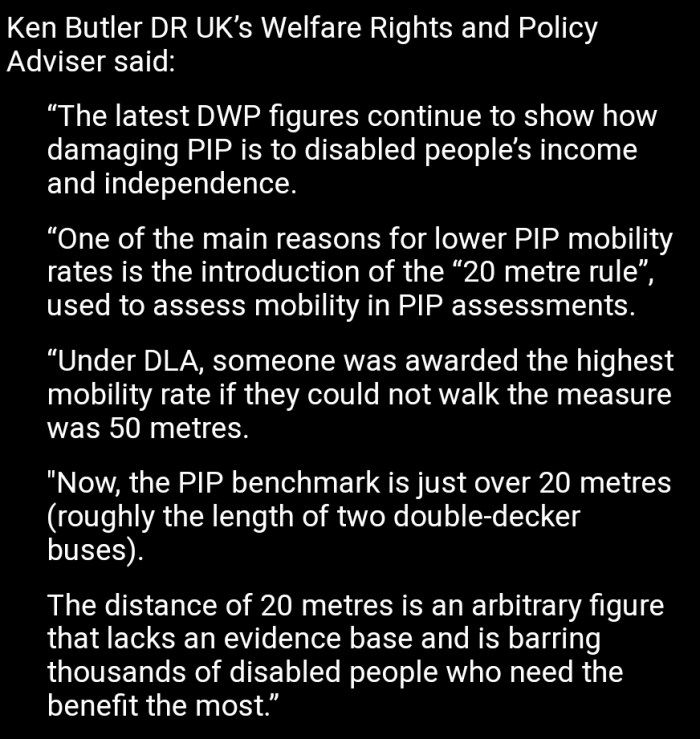
Quotes pictured above are from the incredibly useful Disabity Rights website which can be found here if you’re looking for further information